
New Medicaid initiatives aim to tackle Alabama’s high infant and maternal death rates

MONTGOMERY, Ala. — Leaders at the Alabama Medicaid Agency are hopeful that the state’s infant and maternal mortality rates, which are among the highest in the nation, will start to see improvements after several new initiatives begin rolling out this year.
“Alabama has routinely had high infant mortality rates compared to other states,” said AMA Commissioner Stephanie Azar, speaking with Alabama Daily News Thursday after a meeting of the agency’s Medical Care Advisory Committee in Montgomery.
“It had gotten a little better, (then) I believe the most recent numbers have shown it ticking up a little bit more, but the state of Alabama is initiating multiple initiatives to target that, and maternal health. A lot of infant mortality is tied directly to maternal health.”
According to the most recent data, Alabama had an infant mortality rate of 7.8 deaths per 1,000 births in 2023, a more than 16% increase over the previous year, and more than 39% over the national rate of 5.6 per 1,000. Significant racial disparities among infant deaths were tracked as well, with Black infants more than twice as likely to perish within one year of life when compared to white infants.
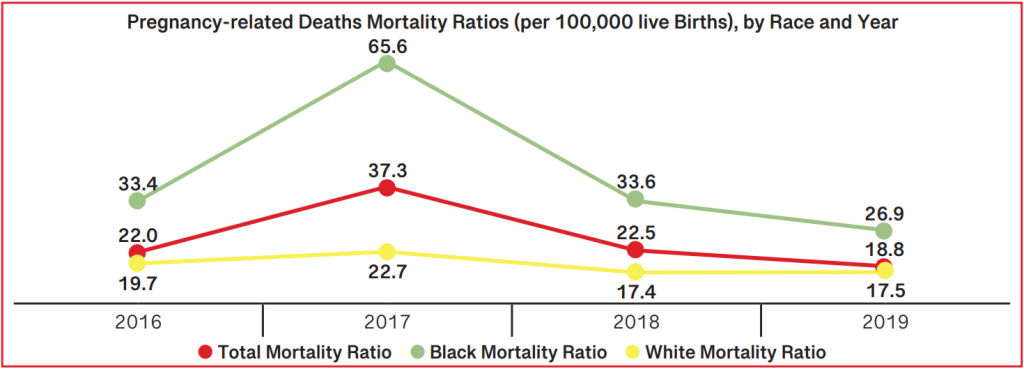
Maternal mortality rates in Alabama aren’t much better. Between 2018 and 2019, the latest available data, there were 93 pregnancy-related deaths for a maternal mortality rate of 29.9 deaths per 100,000 births, more than 64% higher than the national rate of 18.2 per 100,000.
Both the state’s high infant and maternal mortality rates have generally been attributed by public health experts to poverty and a lack of access to health care.
While state leaders have taken stabs at addressing the issue, including awareness campaigns and incentivizing donations to rural hospitals, this year will see the rolling out of several initiatives, among them a federal grant from the Centers for Medicare & Medicaid Services, or CMS, awarded to AMA earlier this year.
“In a highly competitive process, Alabama was fortunate enough to be one of 15 states to be awarded the grant,” said Barry Cambron, who leads the agency’s Department of Health Systems.
“We will be awarded close to $16.5 million from CMS over a ten-year period, and simply put, the overall goal of this project is to improve maternal and child outcomes in this state.”
The grant program is part of the CMS-led Transforming Maternal Health Model, or TMaH, a 10-year initiative aimed out improving health outcomes for Medicaid-enrolled pregnant and postpartum mothers, and will see AMA work in tandem with CMS to improve access, treatment and outcomes for mothers and their newborns through a number of different strategies.
Cambron said that AMA is meeting with CMS representatives weekly, and that stakeholder meetings composed of different maternal care providers are scheduled to kick off in June.

Rolling out this and other initiatives is at least partially contingent on whether additional work and eligibility requirements for Medicaid are implemented at the federal level. Late Wednesday night, the U.S. House passed a multitrillion-dollar tax break package, which included several proposed changes to Medicaid, including new and more strict work, income and residency requirements, as well as a more frequent enrollment period, from once a year to every six months. These changes, the bill’s supporters say, could see federal spending on Medicaid reduced by hundreds of billions of dollars.
With Alabama receiving billions of dollars from the federal government for its Medicaid program, leaders at AMA are keeping a close eye on developments in Washington, D.C., and keeping in constant communication with Alabama’s congressional delegation, Azar said.
“It’s evolving quicker than one can keep up,” she said of the developments in Congress. “One day it’s these types of things are going to occur, and then the other is going to occur. So the one thing I can say, the biggest focus has really turned now to looking at provider assessments, what impact that would have on the state. We’re watching it closely.”
Marsha Raulerson, committee member and representative for the Medical Association of the State of Alabama, said that in her capacity at AMA, which sometimes involves reviewing data on infant deaths, some babies were “falling through the cracks” when it came to a lack of follow ups in instances where an infant may be in danger at home.
“We’ve had a number of deaths of babies going home and nobody ever checked on them, and they died because the parent was drug addicted,” Raulerson said.
“It comes up every time we review deaths, every single time: there’s a baby that went home that was a high-risk baby who was not followed up on. We review 10-15 (infant) deaths every quarter, and there’s always one or two (where the question is) why wasn’t somebody seeing that baby?”
Cambron said that the TMaH model AMA is set to adopt would address that issue given the model’s emphasis on care coordination as a key component.
Another initiative to address infant and maternal mortality being implemented is the Maternal Hypertension Project, also launched in partnership with the CMS. Through the partnership, the two entities will work together to review maternal cardiovascular outcomes in the state, and subsequently, develop a roadmap and action plan to address high-need areas of the state.
Roughly a fifth of all pregnant and postpartum mothers in Alabama are affected by hypertension, or high blood pressure, according to AMA Medical Director Darlene Traffanstedt.
“We looked at two years of data and found that about 20% of our maternity recipients either had a hypertension diagnosis or had pregnancies that were complicated in some way by hypertension,” Traffanstedt told ADN. “That’s a pretty significant number, and it helped drive our decision to join this initiative.”
Late last year, CMS offered an opportunity for Medicaid agencies to participate in one of two affinity groups, or action-oriented collaborative initiatives, one focused on maternal hypertension and cardiovascular health and the other on mental and substance use. Traffanstedt told ADN that AMA opted to participate in the former, given some of the existing initiatives in the state around mental health and substance abuse.
“If you look at the published data from our state’s Maternal Mortality Review Committee, it’s clear that hypertension and hypertension-related diseases contribute significantly to maternal mortality,” Traffanstedt told ADN. “The goal is to design systems that improve outcomes over time.”
A bill signed into law in May was also touted by committee members as being an effective tool to improving infant and maternal mortality in the state, Senate Bill 102. Carried in the Senate by Sen. Coleman-Madison, D-Birmingham, and in the House by Rep. Marilyn Lands, D-Huntsville, SB102 will provide pregnant women presumptive Medicaid eligibility.
Set to go into effect Oct. 1, the bill was designed to speed up the process by which pregnant mothers can start receiving care through Medicaid, as today, coverage does not begin until a Medicaid application is approved, which can take weeks or even months based on factors like income and location.
“The presumptive eligibility for pregnant women, that’s incredibly wonderful news,” Azar told ADN. “They can now get coverage for 60 days, whether they’re ultimately determined eligible for Medicaid or not, as long as they meet the requirements. That means care can start as soon as possible, which helps both the mother and the baby. We’re very excited about that.”
link






