
The biomechanical evolution of the uterus and cervix and fetal growth in human pregnancy

A prospective, time-course, observational study of human pregnancy in participants at low risk for PTB was conducted. Maternal reproductive anatomy, fetal size, and amniotic fluid level were measured via two-dimensional (2D) ultrasound and cervical stiffness using the Pregnolia system (Pregnolia AG, Schlieren, Switzerland). Measurements were collected at four time points during gestation: late first trimester (9w3d–15w3d, w = weeks and d = days), middle second trimester (17w3d–20w5d), late second trimester (23w3d–27w1d), and middle third trimester (33w4d–38w0d). Linear regressions were fit to the data to find relationships with gestational age, and T-tests were performed to analyze the effect of parity. All findings were compared to existing datasets on normal pregnancy.
Study design
This was a prospective observational study of ultrasound dimension and cervical stiffness measurements in participants at low risk for PTB at 9w3d–15w3d, 17w3d–20w5d, 23w3d–27w1d, and 33w4d–38w0d gestation.
Participants
Participants were recruited from prenatal care patients at a single tertiary care center in New York, New York. This study was approved by the Columbia University institutional review board (IRB00002973) and was conducted in accordance with federal guidelines and regulations and the Declaration of Helsinki. All participants provided written informed consent. Participants were approached after being introduced to the study by their primary obstetrician and consented to all study protocols prior to research participation. Fifty participants aged 23–41 were recruited and participated in the study from April 8, 2019, to June 17, 2023. Inclusion criteria included being 18 years of age or older, carrying an uncomplicated singleton gestation, and being able to provide informed consent. Exclusion criteria included a current in-vitro fertilization pregnancy, multifetal reduction, history of PTB, history of cervical surgery, history of cervical shortening in the current pregnancy, history of significant vaginal bleeding during pregnancy, history of any major abdominal/uterine surgery, history of cesarean section, abnormal pap smear, persistent cramping, persistent uterine contractions, vaginal bleeding at the time of consent, uterine anomalies, systemic or vaginal infections at the time of consent, on progesterone in the first trimester, fibroids, placenta previa or abnormal placentation, ovarian cysts (other than a corpus luteal cyst), and anything in vaginal canal in last 24 hours at the time of the first research visit.
Participant age, height, weight, race, ethnicity, patient history, social history, and obstetric history were recorded. At each prenatal research visit, participants reported their weight, pregnancy complications since their last visit, and whether they’d had intercourse or other vaginal transaction in the past 24 hours (tampon, yeast medication, etc.). After the participant delivered, the gestational age at delivery and mode of delivery (cesarean or vaginal) was recorded.
Ultrasound and cervical stiffness measurements
Cervical stiffness was measured using the Pregnolia system (Pregnolia AG, Schlieren, Switzerland). This is an aspiration device administered during a speculum exam. Clinicians were trained to use the device following the “instructions for use” documentation and training videos provided by Pregnolia36. The system is operated via a control unit containing a vacuum pump attached to the probe by flexible tubes. The vacuum is turned on via a foot pedal, creating a negative pressure at the probe head, and the clinician brings the probe head into contact with the distal anterior lip of the cervix. Once contact is established, the clinician slides the probe handle to the middle position, and the negative pressure is increased to pull the cervical tissue 4 mm. The vacuum is stopped at this point, and the pressure required to displace the tissue 4 mm is recorded. The measurement is performed three times. The average of these values is reported as the aCS measurement.
Sonographers trained on the study protocol performed prenatal ultrasound examinations. Ultrasounds were collected by sonographers (I.K., I.M., and V.P.) trained on the ultrasound acquisition protocol by the maternal-fetal medicine specialist who initially developed it (C-L.N-C.). Before imaging, participants were asked to empty their bladders. Ultrasound images were obtained using a GE Voluson E8 (GE Healthcare, Chicago, IL, USA). Standard clinical ultrasonic dimensions of the fetus were measured. Crown-rump length (CRL, [cm]) was measured at time point L1, and EFW [grams] was measured at time points M2, L2, and M3. EFW was calculated using the Hadlock I formula, requiring measurements of biparietal diameter (BPD, [cm]), head circumference (HC, [cm]), abdominal circumference (AC, [cm]), and femur length (FL, [cm])37. The maximum vertical pocket (MVP, [cm]) was collected at all time points, and amniotic fluid index (AFI, [cm]) was collected at time points L2 and M3, and occasionally at M2. Both MVP and AFI provide information on the amniotic fluid level. The placenta location was also recorded at all time points.
With the participant in the supine position, the three B-mode research images of maternal anatomy were acquired: transabdominal (TA) sagittal, TA axial, and transvaginal (TV) sagittal. The TA and TV images were collected following the protocol described in our previous work20. The TA images were acquired using extended field-of-view ultrasound imaging, where the probe was swept across the abdomen, and adjacent images were automatically registered to produce one long image. The extended field-of-view feature permitted imaging of the full length of the uterus in one image. The sonographer acquiring the images placed calipers on the images to mark the location of the dimension measurements at the time of image acquisition. Precise dimension measurements were later taken by E.M.L. using Fiji ImageJ38. Maternal-fetal medicine specialists M.H. and C-L.N-C reviewed images and measurements to verify adequate visualization of the structures under study, including notation of any problematic measurements, such as inaccurate cervical length resulting from a lower uterine segment contraction that distorts the anatomy.
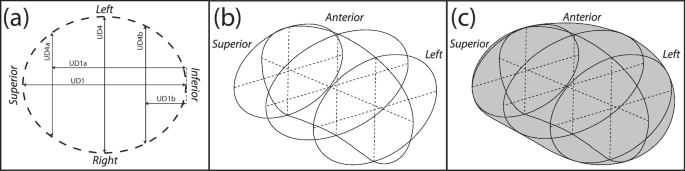
From the TA sagittal ultrasonic image, dimension measurements were collected to characterize the overall shape and size of the sagittal uterus and the placement of the cervix, with dimension measurements used in the statistical analysis having an additional anatomically descriptive label (i.e., IS-UD for the inferior-superior intrauterine diameter) for clarity:
-
UD1 (IS-UD): longest inferior-superior intrauterine diameter, measured from the fundal to the lower uterine segment endometrium (Fig. 5a)
-
UD2: anterior intrauterine diameter, measured perpendicularly from midpoint of UD1 to anterior intrauterine wall (Fig. 5a)
-
UD3: posterior intrauterine diameter, measured perpendicularly from midpoint of UD1 to posterior intrauterine wall (Fig. 5a)
-
UD23 (AP-UD): sum of UD2 and UD3, resulting in the anterior-posterior intrauterine diameter (Fig. 5a)
-
UT1: fundal uterine wall thickness, measured as close to the superior end of UD1 as possible (Fig. 5a)
-
UT2: anterior uterine wall thickness, measured at the anterior end of UD2 (Fig. 5a)
-
PCO: perpendicular cervical offset, perpendicular distance between UD1 and internal os (Fig. 5a)
-
UD3a_eq: posterior dimension perpendicular to UD1 at 25% of UD1 from the superior intrauterine wall (Fig. 5a)
-
UD3b_eq: posterior dimension perpendicular to UD1 at 75% of UD1 from the superior intrauterine wall (Fig. 5a)
-
UD3a_ex: extrema perpendicular distance between posterior wall and UD1 superior to UD3, not always applicable (Fig. 5b)
-
UD1a_ex: distance from inferior end of UD1 to UD3a_ex, only measured if UD3a_ex was measured (Fig. 5b)
-
UD3b_ex: extrema perpendicular distance between posterior wall and UD1 inferior to UD3, not always applicable (Fig. 5b)
-
UD1a_ex: distance from inferior end of UD1 to UD3b_ex, only measured if UD3b_ex was measured (Fig. 5b)

a Measurements collected from sagittal ultrasound images to capture the sagittal uterine shape and placement of the cervix, with measurements of posterior intrauterine diameter taken equidistantly (eq) along UD1. b An alternative method to collecting posterior intrauterine diameter measurements, taken at the superior (UD3a) and inferior (UD3b) extrema (ex). c Measurements collected from axial ultrasound images to capture the axial uterine shape. d Measurements taken from sagittal transvaginal ultrasounds to capture the uterus and cervix. e Measurements of outer cervical diameter taken equidistantly along the cervical length. f Measurements of inner cervical diameter taken equidistantly along the cervical length20,40.
The TA axial ultrasonic image provided the dimensions of the axial uterus:
-
UD4 (LR-UD): longest left-right intrauterine diameter (Fig. 5c)
-
UT3: left/right uterine wall thickness, measured as close to the left or right end of UD4 as possible (Fig. 5c)
Measurements of the cervical size and placement were collected from the TV ultrasonic image:
-
UT4 (LUS-UT): lower uterine segment thickness, measured as the thinnest portion of the visible anterior uterine wall (Fig. 5d)
-
CL: cervical length, measured as the distance between the anatomical internal os (where the anterior and posterior cervix meet in the image) and the external os, inclusive of isthmus length (Fig. 5d)
-
AUCA: anterior uterocervical angle, measured as the angle between the lower uterine segment and cervical canal, placed as 1 cm lines starting at the internal os along the anterior uterine wall and the cervical canal (Fig. 5d)
-
CD1_25: outer cervical diameter measured at 25% of CL from the internal os (Fig. 5e)
-
CD1_50: outer cervical diameter measured at 50% of CL from the internal os (Fig. 5e)
-
CD1_75: outer cervical diameter measured at 75% of CL from the internal os (Fig. 5e)
-
CD2_25: inner cervical diameter measured at 25% of CL from the internal os (Fig. 5f)
-
CD2_50: inner cervical diameter measured at 50% of CL from the internal os (Fig. 5f)
-
CD2_75: inner cervical diameter measured at 75% of CL from the internal os (Fig. 5f)
Estimated uterocervical volume
The estimated uterocervical volume (EUV) was found from solid models generated using the maternal ultrasonic dimensions. Parametric patient-specific CAD models were built in Solidworks 2018–19 (Dassault Systémes, Vélizy-Villacoublay, France) using an existing modeling protocol for all participant visits with ultrasonic dimension measurements (Fig. 6)20.

Three-dimensional solid CAD models of the uterus and cervix for one participant from the late first to middle third trimester with the corresponding ultrasonic images. The top row is the isometric view, and the bottom is the sagittal view. The inferior-superior (IS-UD) and anterior-posterior (AP-UD) intrauterine diameters are marked in the sagittal view.
Several updates to the modeling protocol were made to improve the shape and model build rate. First, due to the variability in sagittal posterior uterine wall shape observed between participants and gestational ages, several methods of building the posterior wall were generated based on parametric measurements collected (updating Fig. 5a in Louwagie et al.20). If both the superior (UD3a) and inferior (UD3b) posterior diameter measurements were collected as extremum (ex), quarter ellipses were used at the inferior and superior ends of the uterus with a spline connecting them through the middle posterior diameter (UD3) (Fig. 7a). A spline was used for the entire posterior uterine profile if no posterior diameters were measured as extremum, thus using the equidistant (eq) approach (Fig. 7b). Finally, if only one of the inferior (Fig. 7c) or superior (Fig. 7d) posterior diameter measurements were collected as extremum, a quarter ellipse was used at the end with the extremum measured, and a spline connecting the middle posterior diameter and equally placed measurement of posterior diameter to the end of the inferior-superior axis.

Method to model the sagittal uterus when a both superior (UD3a_ex) and inferior (UD3b_ex) posterior intrauterine diameters are taken as extrema, b both superior (UD3a_eq) and inferior (UD3b_eq) are taken equidistantly along the inferior-superior axis, c only the inferior (UD3b_ex) is taken as extrema, and d only the superior (UD3a_ex) is taken as extrema. Red arrows depict the ends of the spline, where tangency constraints are enforced.
The method of generating the uterine body was also updated, with an inferior-superior loft through axial profiles used rather than a left-right loft function, updating Fig. 5c in Louwagie et al.20. The coronal uterine shape was still modeled as an ellipse, with elliptical profiles placed coincidentally with UD3a and UD3b (Fig. 8a). The intrauterine diameters at these locations were assigned by their location within the coronal ellipse defined by UD1 and UD4, with UD4a given by Eq. (1) and UD4b given by Eq. (2).
$$\,\textUD4a=2* (\textUD4/\textUD1)* \sqrt\textUD1a* (\textUD1-\textUD1a\,)$$
(1)
$$\,\textUD4b=2* (\textUD4/\textUD1)* \sqrt\textUD1b* (\textUD1-\textUD1b\,)$$
(2)
For the outer uterus, Eq. (1) and Eq. (2) were modified such that the superior and inferior uterus were defined to include uterine wall thicknesses (UT1 and UT4, respectively). The anterior-posterior diameter of the axial elliptical profiles was defined by the sagittal uterine profile (Fig. 8b), and the loft function was executed using the sagittal profile as guides (Fig. 8c).
a Elliptical profiles placed at UD1a, the midpoint of UD1, and UD1b are used as loft profiles, with b the anterior and posterior sagittal outlines used as loft guidelines c resulting in the final uterine body.
The EUV was found using the “Mass Properties” tool within Solidworks.
Statistical analysis
Patient characteristics, intrauterine diameters (IS-UD, AP-UD, and LR-UD), LUS-UT, CL, and aCS were analyzed in RStudio version 1.3.105639. Ultrasound measurements and cervical stiffness were analyzed using a linear regression accounting for differences in both parity and participant. Welch’s t-tests were used to determine measurement differences between cohorts and visits. For the slope comparisons, the hypothesis is that there is no difference between the measurements from the two time points being assessed. The assessed slopes are overall (L1-M3) and between visits (L1-M2, M2-L2, L2-M3). P-values under 0.05 are considered significant and denoted by a star. Means, standard deviations, and regression coefficients were calculated in R. All graphs were created in R.
link







